スポーツ・カイロプラクティック 1st Ray2015.08.11

1st Ray
カイロジャーナル78号(2013.10.25発行)より
機能解剖
第1中足骨頭の足底部には2つの種子骨があります。これらの種子骨は母趾内転筋腱と短母趾屈筋腱の中にあります。その機能は、以下の通りです。1,2,50
- 1st Rayの挙上(第1中足骨の底屈)を促す
- 第1中足骨頭に生じる衝撃を吸収する
- てこの作用により内在筋の機能効率を向上させる
1st Rayに停止を持つ筋肉には、後脛骨筋、前脛骨筋、そして長腓骨筋があります。48,51後脛骨筋の停止は、舟状骨結節、立方骨(足底部)、内側楔状骨、第2~第4中足骨にあります。また、前脛骨筋の停止は、内側楔状骨と第1中足骨底、そして長腓骨筋は第1中足骨底にあります。第1中足骨と内側楔状骨の間の関節(第1足根中足関節)周辺で横足弓と内側縦足弓が交差していることも1st Rayの重要性に関係しています。51
バイオメカニクス
1st Rayは、第1中足骨と内側楔状骨によって構成されており7,16,44、歩行における足部の機能にとって、非常に重要な部分であると言われています。16,39,44従って、1st Rayにおける主要な関節は、第1足根中足関節ということになります。この関節では、矢状断面における運動(底屈と背屈)が主に発生し、それに伴い内反と外反が副次的に起こります。また、1st Rayの運動は、内側楔状骨と舟状骨、内側楔状骨と中間楔状骨、内側楔状骨と第2中足骨(底)、内側楔状骨と第1中足骨(底)の間の関節における可動性から大きな影響を受けることがわかっています。16,23,44特に内側楔状骨と舟状骨の間の関節の運動は、1st Rayの可動性に大きな影響を及ぼしています。
1st Rayは内側縦足弓と連携して、荷重位における重要な衝撃吸収作用を持ちます。つまり、歩行周期の立脚層(表1)において、重要な機能と言うことができます。踵接地において距骨下関節には回内(さらに踵骨の外反)が生じますが、この時、1st Rayの下制が伴います。17,31,38,46それにより、内側縦足弓の安定化が起こります。
- 踵接地(ヒールストライク)
- 足底接地(フットフラット)
- 立脚中期(ミッドスタンス)
- 踵離地(ヒールオフ)
- 足趾離地(トーオフ)
表1 立脚層のフェーズ
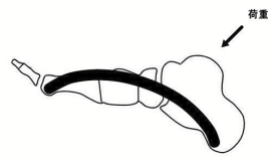
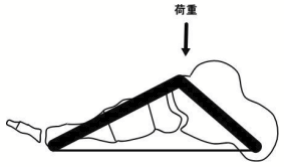
内側縦足弓の安定化機能は、ビーム/トラスメカニズムと呼ばれます。3.8.9.16.48(図1A)。具体的には、踵接地の瞬間(一点支持)、内側縦足弓に挙上方向へ力が作用することで足部の安定化が起こります。一方、トラスメカニズムは、二点支持の状態において、内側縦足弓が安定化するメカニズムのことです(図1B)。足底接地(フットフラット)において、踵骨と中足骨が地面に接地(二点支持)していますが、この時、内側縦足弓はトラスとして機能しています。このように、ビーム/トラスメカニズムでは、1st Rayが内側縦足弓の支柱として作用しています。1st Rayの底屈/背屈に伴う副次的運動について検証している研究も多数存在します。しかし、1st Rayの背屈によって内反が生じたとする研究10.13.16.23.28-30.41.44がある一方、外反が生じたとする研究5.7.18.22.47.51 もあり、運動学的な見解は全く一致しておりません。これらの研究では、1st Rayを局所的かつ他動的に運動させた場合ですが、下腿部の運動との運動連鎖を検証している研究もあります。OldenbrookとSmithらによると、下腿部の内旋に伴い1st Rayでは背屈と外反、下腿部の外旋では、底屈と内反が発生したと報告しています。41また足関節の回内(閉鎖性運動連鎖)では、1st Rayにおいて背屈、さらに内反が生じたとしています。11.29.30しかし、これらの運動連鎖に関しては、研究報告が大変少ないため、この結果を科学的に実証されたものとすることはできません。
一方の手で第2中足骨頭から第5中足骨頭まで固定し、もう一方の手で第1中足骨頭を底屈または背屈させることで、その可動性を検査することができます。第1中足骨頭が底屈位または背屈位の時に、第2中足骨頭との距離を測定します。正常な機能を持つ1st Rayでは、底屈と背屈はほぼ同じ可動域を持っています。44Rootらの研究によると、この距離が底屈位または背屈位の時のいずれも5mmあったと報告されています。43
1st Rayの可動性亢進
1st Rayの可動性亢進は、最初にMortonによって提唱され、その後、多くの研究がなされてきました。35-38.40また、この部位に可動性亢進が生じることで、外反母趾、制限母趾、第5中足骨への負荷の増加などが引き起こされます。6.19.21.25.33.37
第1足根中足関節の背屈方向への安定性にとって、長腓骨筋は大きな影響を及ぼします。4.11.49た、足底部の靱帯(底側足根中足靱帯や底側足根楔状靱帯)や足底筋膜(Windlassメカニズム)も1st Rayの可動性に大きく関与しています。7.17.20.24.32.49
1st Rayの可動性亢進は、足部出生じる様々な疾患の原因となり得ます。40この部位における可動性亢進のサインには、第1足根中足関節の過剰な背屈、内側楔状骨と中間楔状骨の離解、第2中足骨(骨皮質)の肥厚、第2中足趾節関節足底部の皮膚肥厚があります(表2)。35-38.40
- 第1足根中足関節の過剰背屈
- 内側楔状骨と中間楔状骨の離解
- 第2中足骨の肥厚
- 第2中足趾節関節足底部の皮膚肥厚
表2 1st Ray可動性亢進のサイン
このように、1st Rayの可動性亢進は背屈方向へ生じる傾向があります。この原因としては、第1足根中足(Tarsometatarsal; TMT)関節を安定化させている構造の機能低下、または距骨下関節の運動障害が考えられます。歩行周期の立脚中期において、距骨下関節には回内が生じますが、この時、1st Rayには下制が生じ、踵接地における衝撃吸収がなされています。46よって、距骨下関節の運動障害は、1st Rayの運動障害へと連鎖することになります。
第1TMT関節の安定化構造には、関節包靱帯と長腓骨筋(腱)があります。また距骨下関節では、回内障害が問題となる場合が多く見受けられます。この時、踵接地(ヒールストライク)において、踵骨の過剰な外反が生じるため、足底アーチ(内側縦足弓)を適切な状態で維持することが困難になり、足趾離地(トーオフ)の際、第1TMT関節に過剰な背屈が生じるようになります(図2)。また、歩行やジョギング時において、第1TMT関節の過剰背屈が何度も反復されることにより、関節包炎や種子骨炎等の症状へ発展することもあります。

1st Rayの可動性制限
1st Rayの可動域制限は、ほとんどの場合、背屈方向に生じます。1st Rayに正常な可動性がある場合、荷重位において背屈が発生することにより、衝撃吸収作用が機能しますが、背屈方向へ可動域制限がある場合、代償的に近隣関節(第1中足趾節関節など)に可動性亢進が生じる可能性があります。これは、第1中足骨頭の足底側の皮膚に硬結(肥厚)が認められることからも明らかです。34つまり、1st Rayの背屈制限に伴い、第1中足趾節関節の背屈可動性の亢進が生じることで、荷重位(足趾離地)において第1中足骨頭(足底)の皮膚に強い剪断力や圧迫力が加わっていることを意味しています。
また1st Rayの背屈制限に伴い、1st Rayの慢性的な底屈位(サブラクセーション)が生じていることもあります。歩行周期の踵接地から足趾離地にかけて、脛骨には内旋が生じますが、もし1st Rayが底屈位で固定されている場合、脛骨の内旋が著しく制限を受けます。14さらに、距骨下関節の回内、さらに踵骨の外反も制限されるため、衝撃吸収作用が正常に機能しなくなります。
1st Rayと長腓骨筋
長腓骨筋は腓骨頭に起始を持ち、その腱は外果後部、腓骨筋滑車(踵骨)後部、立方骨外側を走行し、第1中足骨底の下外側と内側楔状骨の下内側45.48に停止を持っています。従って、長腓骨筋に適度な緊張が生じることにより、第1中足骨底と内側楔状骨には、外反力が加わり、足底アーチ(特に縦足弓)が扁平化するのを防いでいます(図3)。つまり、長腓骨筋の機能の一つに足底アーチ(特に内側縦足弓)の安定化があります。15.26.27.33.42内側縦足弓は、荷重位において最も重要な足部安定化構造であり8.31.46、1st Rayの機能が大きく影響を及ぼしています。38
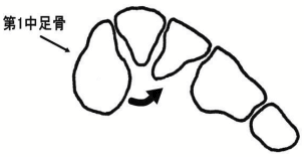
長腓骨筋による第1中足骨底と内側楔状骨への外反作用
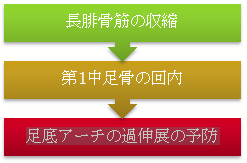
歩行周期の立脚層において、長腓骨筋には伸張性収縮が生じます。これにより、1st Ray(第1中足骨底)には回内(または外反)の負荷が加わり、足底アーチ(縦足弓)の短縮、つまり安定化が起こります。このことは、1st Rayのロッキングメカニズムと呼ばれています(図4)。従って、この筋肉の機能低下は、足底アーチの下制(偏平足)の原因となります。それに伴い、足底筋膜炎(腱膜炎)などの症状へと進行していきます。
また、長腓骨筋は1st Rayの安定化の機能も担っています。44 この機能は特に荷重位において顕著となります。つまり、長腓骨筋は荷重位において、1st Rayの下制(第1足根中足関節の過伸展)を防いでいます。このことは、歩行周期の立脚中期から足趾離地にかけて、長腓骨筋の筋活動レベルが活発化するという研究結果からも裏付けられます。12
また、長腓骨筋は1st Rayが過剰に内転するのも防いでいます。言い換えると、前足の外転を促す機能を持っていることになります。4.49つまり、長腓骨筋は母趾内転筋との拮抗作用を持っており、これは外反母趾と密接に関わりがあることを示唆しています。10.21.25
- 1. Aper R, Saltzman CL, Brown T.: The effect of hallux sesamoid excision on the flexor hallucis longus moment arm. Clin Orthop.;325:209 -217,1996
- 2. Aper RL, Saltzman CL, Brown TD.: The effects of hallux sesamoid resection on the effective moment of the flexor hallucis brevis. Foot Ankle Int. ;15:462- 470,1994
- 3. Birke JA, Franks DB, Foto JG.: First ray joint limitation, pressure, and ulceration of the first metatarsal head in diabetes mellitus. Foot Ankle Int. ;16:277-284,1995
- 4. Bohne WHO, Lee KT, Peterson MGE: Action of the peroneus longus tendon on the first metatarsal against metatarsus primus varus force. Foot Ankle Int 18:510-512,1997
- 5. Broca P: Des difformite´s de la partie ante´rieure des pied produite per l’action de la chaussure. Bull Soc Anat 27:60-62,1852
- 6. Carl A, Ross S, Evanski P, Waugh T: Hypermobility in hallux valgus. Foot Ankle 8:264-270,1988
- 7. D’Amico JC, Schuster RO.: Motion of the first ray: clarification through investigation. J Am Podiatr Assoc 69:17-23,1979
- 8. Dananberg HJ.: Interpreting computerized gait analysis of foot functions, II. Curr Podiatr Med. May :28-30,1990
- 9. Dananberg HJ.: Gait style as an etiology to chronic postural pain, part I: Functional hallux limitus. J Am Podiatr Med Assoc. ;83:433-441,1993
- 10. Ebisui JM: The first ray axis and the first metatarsophalangeal joint: an anatomical and pathomechanical study. J Amer Podiatr Assoc 58:160-168,1968
- 11. Eustace S, O’Byrne J, Beausang O, Codd M, Stack J, Stephens MM.: Hallux valgus, first metatarsal pronation, and collapse of the medial longitudinal arch: a radiological correlation. Skeletal Radiol 23:191-194,1994
- 12. Gra y EG, Basmajian JV: Elect romyography and cinematography of leg and foot (” norma l” and flat) durin g walking. Anat. Rec. 161:1-16,1968
- 13. Grode SE, McCarthy DJ: The anatomical implications of hallux abducto valgus: a cryomicrotomy study. J Am Podiatr Assoc 70:539-551,1980
- 14. Hamill J, Bates BT, Knutzen KM, Kirkpatrick GM.: Relationship between selected static and dynamic lower extremity measures. Clin Biomech. ;4:217-225,1989
- 15. Hammond G: Elevation of the first metatarsal bone with hallux equinus. Surgery 13:240-256,1943
- 16. Hicks JH.: The mechanics of the foot. Part I: the joints. J Anat 87:345-357,1953
- 17. Huang CK, Kitaoka HB, An KN, Chao E: Biomechanical evaluation of longitudinal arch stability. Foot Ankle 14:353-537,1993
- 18. Inman VT: Hallux valgus: a review of etiologic factors. Orthop Clin North Am 5:59-66,1974
- 19. Ito H, Shimizu A, Miyamoto T, Katsura Y, Tanaka K: Clin ical significance of increased mobility in the sagittal plane in patients with hallux valgus. Foot Ankle Int. 20:29-32,1999
- 20. Johnson CH, Christensen JC: Biomechanics of the first ray. Part I: the effects of peroneus longus function. A three-dimensional kinematic analysis in a cadaver model. J Foot Ankle Surg 38:313-321,1999
- 21. Johnson KA, Kile TA: Hallux valgus due to cuneiform-metatarsal instability. South. Orthop. Assoc. 3:273-282,1994
- 22. Kelikian H: Hallux Valgus, Allied Deformities of the Forefoot and Metatarsalgia. pp 31-33, Saunders, Philadelphia,1965
- 23. Kelso SF, Richie DH Jr, Cohen IR, Weed JH, Root ML: Direction and range of motion of the first ray. J Amer Podiatr Assoc 72:600-605,1982
- 24. Kim W, Voloshin AS: Role of the plantar fascia in the load bearing capacity of the human foot. Biomech. 28: 1025-1033,1995
- 25. Klaue K, Hansen ST, Masquelet AC: Clinical quantitative assessment of first tarsometatarsal mobility in the sagittal plane and its relation to hallux valgus deformity. C Foot Ankle Int. 15:9-13,1994
- 26. Langenskiold A, Ritsila V: Supination deformi ty of the forefoot. Acta Orthop. Scand. 48:325-33,1977
- 27. Lapidus PW: “Dorsal bunion” : Its mechanics and operative correction. J. Bone Joint Surg. 22:627-637,1940
- 28. Lundberg A, Goldie I, Kalin B, Selvik G: Kinematics of the ankle/foot complex: plantarflexion and dorsiflexion. Foot Ankle 9:194-200,1989
- 29. Lundberg A, Svensson OK, Bylund C, Goldie I, Selvik G.: Kinematics of the ankle/foot complex-part 2: pronation and supination. Foot Ankle 9:248-253,1989
- 30. Lundberg A, Svensson OK, Bylund C, Selvik G.: Kinematics of the ankle/foot complex-part 3: influence of leg rotation. Foot Ankle 9:304-309,1989
- 31. Manter JT.: Distribution of compression forces in the joints of the human. Anat Rec. ;96:313-321,1946
- 32. McCarthy DJ: The surgical anatomy of the first ray: part II: the proximal segment. J Am Podiatr Assoc 73:1244-1255,1983
- 33. Meyer JM, Tomeno B, Burdet A: Metatarsalgia due to insufficient support by the first ray. Int Orthop. 5:193-201,1981
- 34. Michaud TM.: Foot Orthoses and Other Forms of Conservative Foot Care. Baltimore, Md: Williams & Wilkins; :69-100,1993
- 35. Morton DJ: Evolution of the longitudinal arch of the hum an foot. J. Bone Joint Surg. 6:56 -90,1924
- 36. Morton DJ: Metatarsus atavic us: the iden tification of a dis tinc tive type of foot disorder. J. Bone Joint Surg. 9:53 1-544,1927
- 37. Morton DJ: Hypermobility of the first metatarsal bone. J. Bone Joint Surg. 10:187-196,1928
- 38. Morton DJ: Structural factors in static disorders of the foot. Am. J. Surg. 9:315-328,1930
- 39. Morton DJ.: Dorsal hypermobility of the first metatarsal segment: part III. In The Human Foot: Its Evolution, Physiology, and Functional Disorders, edited by DJ Morton. pp 187-195, Columbia University, New York,1935
- 40. Morton DJ: The Human Foot: lts Evolut ion, Physiology and Functional Disorders. Col umbia Universi ty Press, Morn ingside He ights, NY,1935
- 41. Oldenbrook LL, Smith CE.: Metatarsal head motion secondary to rearfoot pronation and supination: an anatomical investigation. J Am Podiatr Assoc 69:24-28,1979
- 42. Paulos L, Coleman SS, Samuelson KM: Pes cavovarus. J. Bone l oint Surg. 62-A:942- 953,18671979
- 43. Root ML, Orien WP, Weed JH, Hughes RJ.: Biomechanical Examination of the Foot, vol 1. pp 80-87, edited by SA Root, Clinical Biomechanics, Los Angeles,1971
- 44. Root ML, Orien WP, Weed JH.: Motion of the joints of the foot: the first ray. In Clinical Biomechanics. Volume II: Normal and Abnormal Function of the Foot, pp 46-51, 350-354, edited by SA Root. Clinical Biomechanics, Los Angeles,1977
- 45. Salmons S: Gray ‘s Anatomy 38th edition. p. 883, Churchill Livingstone, New York,1995
- 46. Saltzman CL, Nawoczenski DA: Complexities of foot architecture as a base of support. J Orthop Sports Phys Ther. ;21:354-360,1995
- 47. Saltzman CL, Brandser EA, Anderson CM, Berbaum KS, Brown TD: Coronal plane rotation of the first metatarsal. Foot Ankle Int 17:157-161,1996
- 48. Sarrafian SK: Anatomy of the Foot and Ankle. pp.208 – 213, 1.B. Lippincott Co. Philadelphia,1983
- 49. Thordarson DB, Schmotzer H, Chon 1, Peters J: Dynamic support of the human longitudinal arch: a biomechanical evaluation. Clin. Orthop. 316:165-172,1995
- 50. Viladot A.: The metatarsals. In: Wickland E, ed. Disorders of the Foot and Ankle. 2nd ed. Philadelphia, Pa: WB Saunders Co; 1229-1254,1991
- 51. Wanivenhaus A, Pretterklieber M: First tarsometatarsal joint: anatomical biomechanical study. Foot Ankle 9:153-157,1989
