スポーツ・カイロプラクティック 距腿関節のバイオメカニクス2015.09.16

距腿関節のバイオメカニクス
カイロジャーナル83号(2015.6.28発行)より
以下の記事の解説動画をYouTubeにて公開しております。合わせてご利用ください。
1. 基礎医学;距骨の形状
2. 基礎医学;距腿関節の運動軸
距腿関節は距骨(距骨滑車)と脛骨、腓骨(天蓋)との間にできる滑膜性関節です。蝶番関節に分類され、主に背屈と底屈の運動が生じます。可動域は背屈が10°から20°、底屈は20°から50°です。24,43
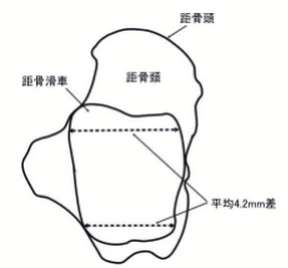
距腿関節の底屈/背屈では、関節のポジションに応じて運動の中心軸と関節の安定性が変化します。その要因の一つに距骨の形状があります。距骨滑車は凸状であり、その表面には前後に溝があります。また、距骨の前方は後方に比べ幅広になっており、平均4.2mmの差があります(図1)。33そのため、距腿関節が底屈位から背屈位へ動いた時、距骨天蓋は1mmから2mm程度広がります。2,8,11,25,38,40,41一方、距骨天蓋は凹状になっており、ここに距骨滑車がかみ合うことで距腿関節の安定性が増加します。7,26,31,42
脛骨、腓骨、距骨は、関節包と靭帯により、それぞれの解剖学的位置関係が維持されています。距腿関節は、外果/内果の近位部分から距骨の遠位部分にかけて関節包により覆われています。この関節包の前部は幅広で薄い膜状になっており、後部は非常に薄く線維は横方向に走行しています。また、関節包の前後部に比べ外側はやや厚みを持っています。17
運動軸
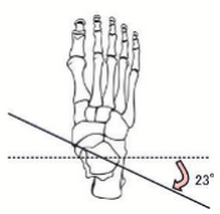
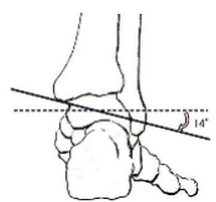
関節が中立位にある時、運動軸は外果と内果下部を結んだ線になります。44外果は内果よりも後下方に位置しているため、運動軸は前額断面から平均23°±9°後方へ傾き、(図2)13,14,22さらに横断面から平均14°±4°下方に傾いています(図3)。4,20従って、足関節の背屈は矢状断面よりも23°外旋位(外転位)、14°内反位(回外位)の面に沿った運動となります。逆に底屈では内旋(内転)と外反の運動(回内)が起こります(表1)。
| 距腿関節 | 実際の運動 |
|---|---|
| 背屈 | 外旋+内反 |
| 底屈 | 内旋+外反 |
脛骨(内果)のバイオメカニクス
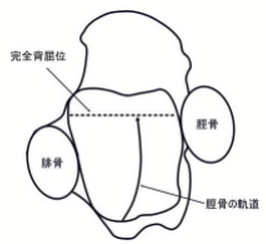
荷重位における距腿関節の背屈では、距骨関節面上で脛骨の前方への滑り運動が生じます(図4)。さらにこの時、脛骨と腓骨の離解に伴い下腿骨間膜が伸張することで、距腿関節の安定性が増します。逆に底屈位において距腿関節の安定性は著しく低下します。このような距骨滑車上の脛骨の滑り運動に伴い、足関節の瞬間中心(Instant center of rotation=ICR)は底屈により後方へ、背屈により前方へ移動します。
底屈位では天蓋は距骨滑車後部にのみ接触しており、下腿骨間膜にも緩みが生じている状態です。このことから、背屈位よりも底屈位において足関節の捻挫が好発することがわかります。
瞬間中心 (Instant center of rotation)
関節運動によって生じる骨の運動が、ある瞬間においてある点を中心に回転運動が生じている場合、その運動の中心点のことを瞬間中心と定義します。
腓骨(外果)のバイオメカニクス
立位(荷重位)において、大腿骨からの荷重負荷のおよそ10%以下が腓骨側に伝わり、残りの90%以上は脛骨側に伝わります。37また、この荷重負荷は距腿関節が背屈位の時に増加し、底屈位において減少します。
腓骨は荷重位における距骨天蓋の安定性維持にとって、重要な役割を果たしています。荷重位において腓骨は平均2.4mm下方へ変位しますが、35腓骨が下方へ変位することで距腿関節は強くかみ合い、下腿骨間膜が緊張(伸張)し外果の安定性が増します。
腓骨の運動は距腿関節と機能的に連動しています。また距骨滑車の形状や距骨の可動性、下腿骨間膜のコンディションなどにより、腓骨の運動は影響を受けます。距腿関節の背屈に伴い腓骨は外方へ動き、底屈に伴い内方へ動きます(X軸、図5)。この運動の可動域は、0.82mmから3mmと幅があります(この運動幅は距骨滑車の形状によります)。6,30
また腓骨は距腿関節の背屈に伴い上方へも変位が起こります(Y軸)。3,9,10,28,35背屈により脛腓靭帯(前・後)と下腿骨間膜が伸張されることで、腓骨を上方へ牽引しています。さらに腓骨は足関節背屈に伴い後方へ、底屈に伴い前方へ変位します(Z軸)。19,32この変位の幅は0.9mmから1.34mmと報告されています。1,19,23,39

| 距腿関節 | X | Y | Z |
|---|---|---|---|
| 背屈 | 外方 | 上方 | 後方 |
| 底屈 | 内方 | 下方 | 前方 |
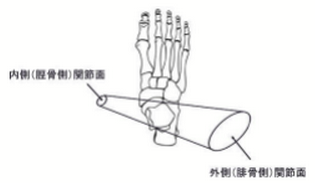
距骨を円錐に見立て、距腿関節と重ねると下図のようになります(図6)。円錐の両端はそれぞれの関節面の向きに合わせて切断されています。36図に示されているように、腓骨の関節面は脛骨側と比べ広く、またやや後方へ傾いています。従って、距腿関節の運動(底屈/背屈)に伴い、腓骨遠位端(外果)は脛骨遠位端(内果)に比べより大きな可動性を持っていることになります。このことは、距腿関節の可動性が腓骨の可動性に大きな影響を受けていることを示唆しています。
距骨のバイオメカニクス
距腿関節において距骨は全体重を支えている唯一の骨です。16,29従って、荷重位において負荷は天蓋から距骨滑車へと伝達されます。距骨滑車へと伝達された負荷は、以下の四方向へと分散されますが、負荷の大部分は距骨下関節を介して踵骨へと伝達されます。
- 舟状骨
- 底側踵舟(スプリング)靭帯
- 載距突起
- 踵骨
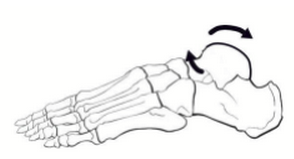
距腿関節の背屈では距骨の後方滑りが生じ(図7) 、底屈では前方滑りが生じています。また、距腿関節の底屈/背屈に伴い距骨には回旋運動も生じます。自動的もしくは他動的な距腿関節の背屈により距骨には外旋が生じ(図8)、底屈により内旋が生じます(表3)。11
| 距腿関節 | 距骨 |
|---|---|
| 背屈 | 後方滑り、外旋 |
| 底屈 | 前方滑り、内旋 |

足関節の捻挫
足関節に捻挫の過去歴がある場合、脛骨、腓骨、距骨には特有の変位が生じています。5,12,15,21,34足関節の捻挫により距腿関節では距骨の前方変位が生じ12、遠位脛腓関節では脛骨に対して腓骨の前方変位が生じる傾向があります。5,15,21,34また、遠位腓骨(外果)において前方変位が生じている場合、近位腓骨(腓骨頭)では後方変位(外旋)が生じています。27従って、距骨には後方滑りの可動域制限が起こり、遠位脛骨には前方滑りの可動域制限が起こります。足関節全体では背屈制限が顕著に起こることになります。5,12,15,21,34
また足関節捻挫の1~11%のケースにおいて、下腿骨間膜の損傷が生じていると言われています。18損傷により下腿骨間膜には線維化・硬化が生じ、腓骨の可動域制限が引き起こされます。既述したように距腿関節の背屈に伴い腓骨と脛骨は離解していきますので、足関節捻挫後の下腿骨間膜の線維化により腓骨の後上方変位、さらに足関節背屈の可動域制限が生じることになります。
参考文献
- Ahl T, Dalen N, Lundberg A, Selvik G: Mobility of the ankle mortise. A roentgen stereophotogrammetric analysis. Acta Orthop Scand; 58: 401–402, 1987
- Anderson MK, Hall SJ: Sports Injury Management. Media, PA: Williams & Wilkins; 217–221, 1995
- Ashhurst APC, Bromer RS: Classification and mechanism of fractures of the leg involving the ankle. Arch Surg; 4: 51-129, 1922
- Barnett C, Napier J: The axis of rotation at the ankle joint in man: Its influence upon the form of the talus and mobility of the fibula. J Anat 86:1, 1952
- Berkowitz MJ, Kim DH: Fibular position in relation to lateral ankle instability. Foot Ankle Int.; 25:318-321, 2004
- Bragonzoni L, Russo A, Girolami M, Albisinni U, Visani A, Mazzotti N, Marcacci M: The distal tibiofibular syndesmosis during passive foot flexion. RSA-based study on intact, ligament injured and screw fixed cadaver specimens. Arch Orthop Trauma Surg; 126:304–308, 2006
- Brand RL, Collins MD: Operative management of ligamentous injuries to the ankle. Clin Sports Med ; 1: 117–130, 1982
- Brosky T, Nyland J, Nitz A, Caborn DNM: The ankle ligaments: considerations of syndesmotic injury and implications for rehabilitation. J Orthop Sports Phys Ther; 21: 197–205, 1995
- Cailliet R: Foot and ankle pain. Philadelphia, F. Davies Company, 1974
- Cedell CA: Ankle lesions. Acta Orthop Stand; 46: 425-445, 1975
- Close JR: Some applications of the functional anatomy of the ankle joint. J Bone Joint Surg Am; 38: 761–781, 1956
- Denegar CR, Hertel J, Fonseca J: The effect of lateral ankle sprain on dorsiflexion range of motion, posterior talar glide, and joint laxity. J Orthop Sports Phys Ther; 32: 166-173, 2002
- Elftman H: The orientation of the joints of the lower extremity. Bull Hosp Joint Dis 6: 139-143, 1945
- Elftman H: The transverse tarsal joint and its control. Clin Orthop 16: 41-45, 1960
- Eren OT, Kucukkaya M, Kabukcuoglu Y, Kuzgun U: The role of a posteriorly positioned fibula in ankle sprain. Am J Sports Med; 31:995-998, 2003
- Frigg A, Magerkurth O, Valderrabano V, Ledermann HP, Hintermann B: The effect of osseous ankle configuration on chronic ankle instability. Br J Sports Med; 41: 420–424, 2007
- Goss CM, ed: Gray’s Anatomy. 29th American ed. Philadelphia, PA: Lea & Febiger; 349–369, 1973
- Grass R, Herzmann K, Biewener A, Zwipp H: Injuries of the inferior tibiofibular syndesmosis. Unfallchirurg ; 103: 520–532, 2000
- Henkemeyer H, Puschel R, Burri C: Experimental studies on the biomechanics of syndesmosis. Langenbecks Arch Chir Suppl; 369–371, 1975
- Hicks J: Mechanics of the foot 1: The joints. J Anat 87: 345, 1953
- Hubbard TJ, Hertel J, Sherbondy P: Fibular position in individuals with self-reported chronic ankle instability. J Orthop Sports Phys Ther; 36: 3-9, 2006
- Isman R, Inman V: Arthropometric studies of the human foot and ankle. Bull Prosthet Res 10/11: 97-129, 1969
- Jend HH, Ney R, Schottle H: Movements of the fibula. Unfallchirurg; 90:144–147, 1987
- Kapandji I: The Physiology of the Joints, 5th ed. Baltimore, Williams & Wilkins, 1987
- Katznelson A, Lin E, Militiano J: Ruptures of the ligaments about the tibio-fibular syndesmosis. Injury; 15: 170–172, 1983
- Mack RP: Ankle injuries in athletics. Clin Sports Med; 1: 71–84, 1982
- Ogden JA: The anatomy and function of the proximal tibiofibular joint. Clin Orthop Relat Res; 101-103, 1974
- Oglivie-Harris DJ, Reed SC, Hedman TP: Disruption of the ankle syndesmosis: biomechanical study of the ligamentous restraints. Arthroscopy; 10: 558–560, 1994
- Pal GP, Routal RV: Architecture of cancellous bone of the human talus. Anat Rec; 252: 185–193, 1998
- Peter RE, Harrington RM, Henley MB, Tencer AF: Biomechanical effects of internal fixation of the distal tibiofibular syndesmotic joint: comparison of two fixation techniques. J Orthop Trauma; 8:215–219, 1994
- Pick TD, Howden R: Gray’s Anatomy, Descriptive and Surgical. New York, NY: Bounty Books; 283–286, 1977
- Reimann R, Anderhuber F: Compensatory movements of the fibula necessitated by the wedge shape of the trochlea tali. Acta Anat (Basel); 108:60–67, 1980
- Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional. 2nd ed. Philadelphia, PA: JB Lippincott; 159–187, 474–551, 1993
- Scranton Jr PE, McDermott JE, Rogers JV: The relationship between chronic ankle instability and variations in mortise anatomy and impingement spurs. Foot Ankle Int; 21: 657-664, 2000
- Scranton PE, McMaster JF, Kelly E: Dynamic fibular function: a new concept. Clin Orthop;118:76–81, 1976
- Seber S, Hazer B, Kose N, et al: Rotational profile of the lower extremity and foot progression angle: Computerized tomographic examination of 50 male adults. Arch Orthop Trauma Surg 120: 255-258, 2000
- 37. Segal D, Pick RY, Klein HA, et al.: The role of the lateral malleolus as a stabilizing factor of the ankle joint: Preliminary report. Foot Ankle 2: 25-29, 1981
- Stiehl JB: Complex ankle fracture dislocations with syndesmotic diastasis. Orthop Rev; 19:499–507, 1990
- Svensson OK, Lundberg A, Walheim G, Selvik G: In vivo fibular motions during various movements of the ankle. Clin Biom; 155–160, 1989
- Taylor DC, Englehardt DL, Bassett FH III: Syndesmosis sprains of the ankle: the influence of heterotopic ossification. Am J Sports Med; 20: 146–150, 1992
- Taylor DC, Bassett FH: Syndesmosis ankle sprains: diagnosing the injury and aiding recovery. Physician Sportsmed; 21(12): 39–46, 1993
- Thompson CW, Floyd RT: Manual of Structural Kinesiology. 13th ed. Dubuque, IA: WCB/McGraw-Hill; 129–132, 1988
- Williams P: Gray’s Anatomy, 38th ed. New York, Churchill Livingstone, 1995
- Woollacott M, Shumway-Cook A: Atention and the control of posture and gait: A review of an emerging area of research. Gait Posture 16: 1, 2002
